Glaucoma & Pseudoexfoliation
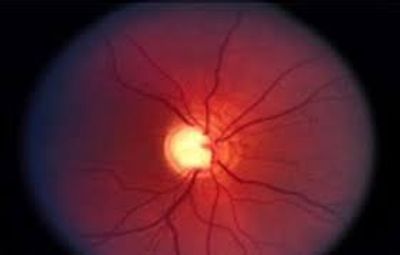
Glaucoma is a disease of the eyes where there is an increased pressure (intraocular pressure) inside the eye. The increased pressure damages the optic nerve, which connects the eye to the brain. The damage to the optic nerve and adjacent retina causes permanent loss of vision, first peripherally and eventually the central vision is lost.
There are two main types of glaucoma. The rare type is called narrow angle or acute angle closure glaucoma. By far, the most common type of glaucoma is called open angle glaucoma. Open angle glaucoma is often called a silent thief of vision, because most people have no signs or symptoms of this disease till they lose a lot of vision. Approximately 2.2 million Americans have open angle glaucoma, and about 120,000 are blind from it. Pseudoexfoliation glaucoma is the most common type of open angle glaucoma, accounting for over 10% of cases of open angle glaucoma. That means there are over 220,000 people with pseudoexfoliation glaucoma in the USA.
Pseudoexfoliation glaucoma or elevated intraocular pressure is caused by the pseudoexfoliation flakes clogging the trabecular meshwork of the eye, and preventing fluid inside the eye from draining out properly. Not all eyes with pseudoexfoliation need to be treated, but if the intraocular pressure is elevated significantly, pseudoexfoliation glaucoma tends to be the most difficult glaucoma to treat, because it often causes very high pressures, which respond poorly to the standard glaucoma medications or eye drops. Therefore, pseudoexfoliation glaucoma must be monitored carefully and frequently to prevent permanent loss of vision. Some cases of pseudoexfoliation glaucoma are misdiagnosed as standard open angle glaucoma because the eye doctor does not notice the pseudoexfoliation flakes on the surface of the pupil and the lens. In order to diagnose pseudoexfoliation glaucoma, the surface of the lens has to be examined with a slit lamp AFTER dilation of the pupil with eye drops, since the pseudoexfoliation flakes are sometimes very tiny, subtle and impossible to see without pupil dilation.
Most cases of pseudoexfoliation glaucoma are treated with eye drops. There are a variety of categories of drops that can be used, but the treatment must be carefully customized for each patient since every eye responds differently and variably to the glaucoma eye drops. Prostaglandin eye drops (Xalatan, Latanoprost, Travatan-Z, Lumigan, Rescula) are the most common initial drops used to treat the high intraocular pressure in pseudoexfoliation glaucoma. These drops don't cure the condition, but they do lower the pressure in the eye and prevent damage to the optic nerve and loss of vision. If prostaglandin drops don't work well enough, patients are often treated with additional drops such as alpha-adrenergic agonists (Alphagan, Brimonidine, Iopidine), beta-blocker drops (Timoptic, Betoptic, Timolol), carbonic anhydrase inhibitors (Azopt, Dorzolamide, Trusopt), and rarely cholinergic agonists (Pilocarpine). Each of these drops has its own safety and side effect profiles, and various pros and cons. Every eye responds differently to each drop. Some of the drops can also cause systemic side effects such as effects on the heart rate, blood pressure, mood, sleep cycle, and other body functions. In more severe cases oral carbonic anhydrase medications (Diamox, Neptazane, Acetazolamide) are used to lower the intraocular pressure. These medications can have significant risks and side effects as well, but may be necessary to prevent vision loss.
If the various eye drops and/or pills do not adequately lower the intraocular pressure in cases of pseudoexfoliation glaucoma, then the eye is often treated with a laser procedure called argon laser trabeculoplasty, or selective laser trabeculoplasty. This relatively safe procedure opens up the pseudoexfoliation flake-clogged trabecular meshwork and lowers the intraocular pressure in most cases. The procedure may need to be repeated several times, but in severe or resistant cases of pseudoexfoliation, the laser procedure benefit is sometimes short lasting.
If eye drop and laser treatments have not sufficiently lowered the intraocular pressure to a safe level, then eyes with pseudoexfoliation glaucoma require glaucoma filtering surgery (trabeculectomy, shunt procedures) to lower the intraocular pressure. These surgeries are a last resort since they carry significant additional risks, but often are effective.
Patients with pseudoexfoliation glaucoma need to be carefully monitored by ophthalmologists to make sure that their intraocular pressures are sustained at a safe level. There is no safe pressure level that is good for every eye. Some eyes tolerate relatively high intraocular pressures without loss of vision, and other eyes lose vision with relatively low intraocular pressure levels. To determine if the intraocular pressure level is “safe” for each specific eye, ophthalmologists will monitor the health of the retina and optic nerve using sophisticated scanning equipment known as OCT and HRT. Additionally, ophthalmologists carefully monitor the eye's peripheral vision by performing a Visual Field test from time to time – Humphrey Visual Field testing is considered to be the benchmark, standard test. Additionally the eye's corneal thickness must be measured, since eyes that have thin corneas are more prone to damage from elevated intraocular pressure, especially if the eye has pseudoexfoliation.
Frequent and careful monitoring of these multiple parameters or tests, and treatment with the best eye drop, pill, laser or surgery combination is critical to prevent permanent loss of vision from pseudoexfoliation. Ophthalmologists who are experienced with the treatment of pseudoexfoliation glaucoma are very familiar with the various diagnostic and treatment modalities and can explain it to their patients who have this condition.